
TRAUMATIC BRAIN INJURY TBI Clinical Mgt. PowerPoint Presentation on CD For Sale

When you click on links to various merchants on this site and make a purchase, this can result in this site earning a commission. Affiliate programs and affiliations include, but are not limited to, the eBay Partner Network.

TRAUMATIC BRAIN INJURY TBI Clinical Mgt. PowerPoint Presentation on CD:
$12.99
Thank you!
If you do not wish to have your item(s) delivered on data disc(s), I can provide them on a flash drive and other means as well. Just let me know if a disc does not work for you and we can discuss delivery by other methods.
COMBINING SHIPPING COSTS
Are you purchasing multiple items? I will: a) combine all invoices before payment and charge shipping equivalent to one item, or b) refund all shipping costs in excess of one item after payment.
All derivative (i.e. change in media; by compilation) work from this underlying U.S. Government public domain/public release data is COPYRIGHT © GOVPUBS$3.00 first class shipping in U.S.
Includes the Adobe Acrobat Reader for reading and printing publications.
Numerous illustrations and matrices.
Contains the following key public domain (not copyrighted) U.S. Government publication(s) on one CD-ROM in both Microsoft PowerPoint and Adobe Acrobat PDF file formats:
TITLE: CLINICAL MANAGEMENT OF TRAUMATIC BRAIN INJURY, 69 pages (slides)
SLIDE TOPICS, SUBTOPICS and CONTENTS:
CLINICAL MANAGEMENT OF TRAUMATIC BRAIN INJURY
Geoffrey S.F. Ling, M.D., Ph.D.
Lieut. Col, Medical Corps, U.S. Army
Director, Neuro Critical Care
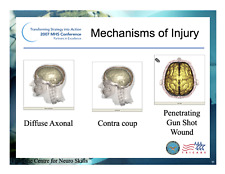
Head Trauma
Plain Films
Skull fracture (esp, if fx is perpendicular to plain of CT imaging
Foreign body localization
CT
Bony, extracranial soft tissue, brain, acute blood
Blood may be low or iso-dense making it harder to dx (occurs in anemia and DIC)
MRI
Superior to CT
Data provided is not necessarily more clinically relevant
Much better for DIA and posterior fossa lesions
Plain X-rays in Head Trauma
Assess bony calvarium
Fracture identification
Limited utility
Good for identifying fractures that are perpendicular to plain of CT imaging
As these can be missed by CT
Optimal Study
AP, Lateral
+/- tangentialCT in Head Trauma
Most useful imaging tool
Identifies bony and soft tissue lesions
Blood, edema, air
Foreign bodies
Weakness
Acute blood may be low or iso dense in anemia or DIC
Not as good as MRI for DAI, cortical contussion, posterior fossa pathology
Miss fracture at vertex and traumatic aneurysms
Zee and Go, Neuroimaging Clinics N Amer 8:525 (1998)CT in Head Trauma Optimal Study
CT w/o contrast
Slices: 8-10 mm
Smaller in areas of greater concern, ex. skull base
Image in brain window
Image in bone window
+/- image in subdural window
Settings: center 60Hu, width 120Hu
Mirvis and Shanmuganathan J Intens Care Med 9:305 (1994)
CT and Increased ICP
CT has high sensitivity for detecting high ICP (99%)
CT has lower specificity (78%)
Radiologists diagnose increased ICP on anatomic changes: tissue density, fluid compartment shifts, gray/white jxn changes, herniation
Conclude: High false positive may lead to inappropriate interventions to reduce ICP
Hirsch et al, Pediatr Radiol 30: 439 (2000) Indications for CT in Head Trauma
GCS < 15
Clinical evidence of basilar skull fx
Depressed skull fx > 1 cm
Penetrating injury
Anisocoria or fixed and dilated pupils
Neurological deficit
Known bleeding diathesis or anticoagulant tx
Prolonged LOC (> 5 min)
Antegrade amnesia
Zee and Go, Neuroimaging Clinics N Amer 8:525 (1998)
Indications Based on Risk
High Risk for intracranial pathology (need CT)
Focal neurol signs, penetrating wound, depressed skull fx (palpable), impaired MS (no drugs, intoxicants)
Moderate Risk (possible CT)
Hx of changed MS, progressive h/a, sz, amnesia, clinical evid of basilar skull fx, serous facial injury, vomitting, multiple trauma, possible child abuse, < 2 y.o.
Low Risk (no CT)
Asymptomatic, headache, dizziness, scalp lac or hematoma
Mirivs and Shanmuganathan, J Intens Care Med 9:305 (1994)
Masters et al, New Engl J Med 316:84 (1987)
MRI in Head Trauma
MRI is superior to CT for every pathology except skull fracture and acute subarachnoid hemorrhage
Much superior for edema, DAI, contusions and hematomas (> 30% better for SDH and EDH), posterior fossa lesions
Less advantageous
Speed of study, ability to image bones, abdomen and chest at the same sitting
Improved data does not impact clinical care
Bruce, Child Nerv Syst 16: 755 (2000)
Orrison et alm Am J Neurorad 15: 351 (1994)
Zimmerman & Bilaniuk, Neuroimag Clin N Amer 4:349 (1994)MRI in Acute Head Trauma
Standard brain MRI using T1 and T2 sequences
Axial and sagittal planes
DWI, FLAIR and gradient echo images
MRA for vascular examinationsClosed Head Injury
Lateral Skull X-ray
CT Head
Gunshot Wound
Plain X-ray of GSW
CT of GSW
Knife Wound
Plain X-ray Knife Wound
CT Knife Wound
Goals of Management
Maintain general physiology
Treat immediate consequences of primary injury
Minimize secondary CNS injury
treat edema and elevated ICP
maintain cerebral perfusion pressure
Indications for ICP MonitoringSevere TBI (GCS < 8) and abn CT
Severe TBI and normal CT if (>2):
> 40 years old, uni or bilateral motor posturing, systolic BP < 90 mmHg
Other clinical indications
Marmarou et al, J Neurosurg 75:S59-S66 (1991)
Gopinath et al, J N Nsurg Psy 57:717-723 (1994)
Eisenberg et al, J Neurosurg 69:15-23 (1988)
Intracranial Pressure TBI
Threshold for intervention is recommended to be 20-25 mmHg
Clinical neuro examination and appropriate CT imaging must also be followed
Adequate CPP must be maintained
ICP Threshold for Intervention
In pts without craniectomy, an ICP threshold of 25 mmHg improved outcome.
craniectomy pts, ICP threshold 15 mmHg
Using logistic regression analysis of pts in the TBI Databank, 20 mmHg was found to correlate with best outcome.
Eisenberg et al, J Neurosurg 69:15-23 (1988)
Marmarou et al, J Neurosurg 75:S59-S66 (1991)
Cerebral Perfusion PressureCerebral perfusion pressure should be maintained at > 70 mm Hg
Goal is to optimize cerebral perfusion
Minimize regional and global ischemiaCerebral Perfusion PressureCPP = MAP - ICP (+ CVP)
Pressure gradient driving CBF and metabolite /oxygen delivery
Cerebral Perfusion Pressure in TBI
Prospective studies have shown 50% increase in survival
50% increase in “good” outcome
No increase in ICP or adverse clinical outcomes by actively maintaining CPP
Marion et al, J Neurosurg 75:354-362 (1993)
Marshall et al, J Neurosurg 75:S28-S36 (1991)
Cerebral Perfusion Pressure in TBI
Retrospective studies have shown that there is 20% increased mortality for each incremental decrease of 10 mmHg
For CPP < 60 mmHg greater than 33% of the time, 100% mortalityChangaris et al, J Trauma 27:1007-1013 (1987)
Clinical Approach to CPP
Goal > 70 mmHg
Normalize intravascular volume
+/- hypertonic saline
Pharmacologically induce systemic hypertension
Requirements
ICP monitor, arterial line, +/- PA catheter
Hyperventilation Paradox in TBI
Aggressive hyperventilation (PaCO2<25 mmHg) can cause a rapid reduction in ICP
a therapeutic goal
HV can increase jugular venous desats
assoc with poor outcome
HV can incr AVdo2 and decrease CBF
potentially exacerbating ischemia
Hyperventilation Use in TBI
For acute ICP management, begin with a PaCO2 goal of 30-35 mmHg
For recalcitrant ICP, advance PaCO2 goal to 25-30 mmHg
consider use of a jugular bulb catheter
Taper HV as soon as possible
Chronic HV should be avoided, particularly in the first 24 Hrs
Mannitol Use in TBI
Dose: 0.25 - 1 gm/kg, i.v. bolus
Use bolus dosing
Maintain intravascular volume
Maintain serum Osm < 320 mOsm/L, particularly if renal failure is possible
Mannitol Mechanisms of Action in TBIRheologic
Plasma expansion
Osmotic
producing gradient
Mannitol Plasma Expansion Effect
Almost immediate onset of action
clinical effect within minutes
Optimal rheologic effects
reduces HCT which reduces viscosity
increase CBF which increase O2 delivery
Best accomplished with bolus dosing
Barry et al, NEJM 264:1085-1088 (1961)
Mendelow et al, J Neurosurg 63:43-48 (1985)
Mannitol Positive Osmotic Effect
Delayed onset but persistent effect
onset 15-30 min & persists approx 6 hours
Establishes osmotic gradient between plasma and cells
May reduce edema
Cruz et al, J Neurosurg 73:725-730 (1990)
McGraw& Howard, Neurosurg 13:269-271 (1983)
Nath & Galbraith, J Neurosurg 65:41-43 (1986)
Mannitol Negative Osmotic EffectOpens BBB and can sequester in brain
can lead to exacerbation of ICP & edema
Risk of ATN (esp if serum osm > 320)
Potential cardiovascular compromise
rare in actual clinical practice
Cruz et al, J Neurosurg 73:725-730 (1990)
McGraw& Howard, Neurosurg 13:269-271 (1983)
Mannitol Effectiveness in TBI
Superior to barbiturate for control of ICP and CPP
Significantly better survival
Reduction of edema after low dosesSchwartz et al, Can J Neurol Sci 11:434-440 (1984)
Nath & Galbraith, J Neurosurg 65:41-43 (1986)
Barbiturate Coma TBI
Barbiturate coma may be considered for pts in whom intracranial hypertension remains refractory to maximal medical and neurosurgical interventions
Basic Premise
absolute ICP control improves outcome
Barbiturate Mechanism of Action
Suppress cerebral metabolism
Reduce cerebral blood flow and thus cerebral blood volume
Alter vascular tone
Inhibit free radical mediated lipid perioxidation
Results in reduced ICP and optimized perfusion
Pentobarbital Dosing
Loading Dose
10 mg/kg i.v. over 30 minutes
5 mg/kg i.v. every hour X 3 doses
Maintenance Dose
1 mg/kg/hr, i.v. infusion
Pentobarbital Dosing Goals
Therapeutic levels: 3-4 mg%
poor correlation with therapeutic benefit
EEG burst suppression
most reliable form of monitoring
maximal reduction of cerebral metabolism and CBF
ICP < 20 mmHg
Eisenberg et al, J Neurosurg 69:15-23 (1988)
Pentobarbital Therapy in TBI
Improved survival when used to treat recalcitrant intracranial hypertension in hemodynamically salvageable severe TBI pts.
Patient selection is crucial
pts who failed other ICP therapy
pts with adequate cardiovasc fxn
pts w/ intact autoregulation
pts without diffuse injury
Pentobarbital Ineffective Conditions
Pts with impaired cerebral vasoreactivity/autoregulation
Pts with diffuse injury
Pts with pre-existing hypotension
As prophylactic tx of ICP
Nordstrom et al, J Neurosurg 68:424-431
Lobato et al, J Neurosurg 68:417-423
Malignant ICP
Up to 15% of TBI pts will not respond to either maximal medical or neurosurgical intervention.
Mortality in these pts approaches 100%Miller et al, J Neurosurg 54:289-299 (1981)
Narayan et al, J Neurosurg 56:650-659 (1982)
Hypertonic Saline
0.9% to 3% to 27% NaCl solutions
Shown to be effective in neurotrauma by shrinking brain and thus reduce ICP
can do so and maintain intravascular volume
Goal is to increase osmolarity not dehydrate
May not be effective in stroke
Qureshi and Suarez, Crit Care Med 28: 3301 (2000)
Bhardwaj et al, Stroke 31: 1694 (2000)
Munar et al, J Neurotrauma 17: 41 (2000)
Hypertonic Saline Clinical Approach
Establish central venous access
Initiate therapy with 3% saline at 75 cc/hr (or higher if requiring fluid resuscitation)
use 50% chloride/50% acetate to minimize risk of hyperchloremia
Infuse to a goal Na (ex. 145-150)
Check serum Na frequently (q 4-6 hrs)
“ballpark” serum osm will be double serum Na
Hypertonic Saline Clinical Approach
Reassess neuro exam, increase Na goal as needed (max: 160-165)
When goal is achieved, continue infusion with 0.9% saline (or 2% if Na drifts downward)
Continue treatment until day 4 or 5 post-injury
To stop, just d/c hypertonic saline infusion and allow pt to autotaper to stop acute seizure
phenytoin (Dilantin) as prophylaxis
AEDs in TBI
Phenytoin or carbamazepine are effective in preventing early post-traumatic seizures.
Phenytoin, carbamazepine and other AEDs have not been shown to be effective in preventing late post-traumatic seizures
Posttraumatic Seizures
Classification of seizures
Early: occurring within 7 days of injury
Late: occurring after 7 days following injury
Incidence
early PTS: 4-25%
late PTS: 9-42%
50% pts will develop szs after penetrating injury
Temkin et al, Neurosurg Clin 2:425-435 (1991)Posttraumatic Seizures Risk Factors
Penetrating head wound
Hematoma
subdural, epidural, parenchymal
Depressed skull fracture
Cortical contusion
GCS < 10
Seizure within 24 hr of injury
Posttraumatic Seizure Therapeutic Goals
Prevention of early PTS may avoid further compromising an injured brain.
exacerbation of ICP, CBF, O2 delivery and consumption, NT release
Prevention of early PTS may prevent the development of late PTS.
Based primarily on expt studies of kindling
Not supported in clinical studies
Early Posttraumatic Seizures AEDsPhenytoin therapy leads to a significant reduction in early PTS
Carbamazepine therapy leads to a significant reduction in early PTSTemkin et al, NEJM 323:497 (1990)
Glotzner et al, Neurochir 26:66-79 (1983)
Late Posttraumatic Seizures AEDsPhenytoin, carbamazepine and phenobarbital therapies did not significantly reduce the rate of late PTSTemkin et al, NEJM 323:497 (1990)
Glotzner et al, Neurochir 26:66-79 (1983)
Manaka et al, JpnJ Psych Neuro 46:311-315 (1992)
Fever and Shivering
Both conditions increase metabolic demand and worsen paralysis (sedate pt concurrently)
cisatracurium (Nimbex): 0.2mg/kg then 1 - 3 mcg/kg/min
vecuronium: 0.1 mcg/kg then 1 mcg/kg/minOther Therapies
Furosemide
Hypertonic intravascular fluids
Torosemide
Barbiturate coma
Acetozolamide
Emerging Therapies
NMDA antagonist
Calcium channel blockers
Antioxidants
Free radical scavengers
Anti-inflammatory agents
Other Emerging TherapiesHypothermia
Failed clinical trial
Hyperosmotic resucitation fluids
Hibernation
Steroids Use in TBI
The use of glucocorticoids is not recommended for either improving outcome or reducing ICP.
Methylprednisolone TBINo significant change in ICP
50% incidence of GI bleed and 85% incidence of hyperglycemia
No significant difference in outcome
doses up to 100 mg/kg/day Gudeman et al, J Neurosurg 51:301-306 (1979)
Giannotta et al, Neurosurg 15: 497-501 (1984)
Dexamethasone TBI
No significant difference in either 1 month survival or 6 month outcome
increased hyperglycemia, which correlated to adverse outcome
doses up to 100 mg/day
No significant difference in ICP
Braakman et al, J Neurosurg 58:326-330 (1983)
Dearden et al, J Neurosurg 64 :81-88 (1986)
Lam et al, J neurosurg 75:545-551 (1991)
Other Adjunctive TherapyDVT prophylaxis
Ulcer prophylaxis
Decubitus ulcer prophylaxis
Pharmacologic Therapy Not Routinely RecommendedSedation
interferes with neurologic exam and thus treatment
Neuromuscular Blockade
assoc w/ incr length of stay, incr incidence of pneumonia and sepsis
no improvement in outcome
Hsiang et al, Crit Care Med 22:1471-1476 (1994)
Hypothermia in TBIModerate hypothermia (33oC) may hasten recovery among a subset of severe TBI pts
GCS 5-7 pts benefited but more severely injured pts did notMarion et al, NEJM 336:540-546 (1997)
Nutritional Support
Replace 140% of resting metabolism expenditure in nonparalyzed pts
Use formulas containing at least 15% calories as protein by 7 th day after TBI
Enteral feeds are preferable
less hyperglycemia, less infxn, cheaper
jejunal feeding may be superior
Nutritional Support in TBI
In first 2 weeks, pts are hypermetabolic
TBI pts lose approx 15% of body wt/week from nitrogen loss
30% wt loss increases mortality
Degrees of Certainty
Standards
principles of pt management with a high degree of clinical certainty
Guidelines
moderate degree of clinical certainty
Options
unclear clinical certainty
Clinical Monitoring of TBI SummaryICP monitoring (guideline)
ICP Goal < 20-25 mmHg (guideline)
CPP goal > 70 mmHg (option)
During HV, consider Sjo2, AVdo2 and CBF monitoring (Option)
Clinical Therapy in TBI Summary
Mannitol therapy as boluses (guideline)
Acute hyperventilation (option)
Barbiturate coma for intractable ICP (guideline)
AEDs for early PTS (guideline)
Nutritional support (guideline)
jejunal feeding preferentially (option)
Therapies to Avoid in TBI Summary
Chronic hyperventilation without increased ICP (standard)
Prophylactic HV (guideline)
AEDs for late PTS (standard)
Prolonged paralysis (option)
Sedation (option)
Related Items:

Rare Advanced Combat Helmet ( ACH ) Traumatic Brain Injury ( TBI ) sensor LARGE
$279.97
42 page TRAUMATIC BRAIN INJURY Primer PowerPoint Presentation on CD
$12.99
Lot of 10 Green Ribbon TBI Traumatic Brain Injury Pinback Button Pins 1.25"
$15.95